When Diastasis Recti Shows Up as Back, Neck, or Shoulder Pain
Most people assume diastasis recti is a short‑term postpartum issue. (NIH – J Sports Med. 2016)
Something that happens during pregnancy, gets a little attention at a six‑week checkup, and then either “goes away” or just becomes part of the background noise of life.
In practice, that’s often not what happens.
One of the most common patterns we see in the clinic is unrecognized diastasis recti showing up years—or even decades—later as chronic back pain, neck tension, shoulder issues, or recurring injuries that never quite resolve.
Many clients don’t come in asking about their core at all. They come in for plantar fasciitis, low back pain, or stubborn shoulder tension. The missing piece is often a split they didn’t know existed—or assumed was no longer relevant.
What Diastasis Recti Actually Is (and Why It Persists)
Diastasis recti occurs when the two sides of the rectus abdominis separate along the midline, creating a gap in the connective tissue known as the linea alba. (Cleveland Clinic)
What’s important—and frequently misunderstood—is that the linea alba behaves far more like a ligament or tendon than a muscle. It does not “strengthen” quickly, and it does not respond well to force.
That’s why aggressive core exercises often make things worse.
If excessive tension continues to pull on the tissue, the split remains—even if years have passed since pregnancy. Without proper unloading and support, the body simply adapts around the separation.
And it adapts in ways that tend to hurt.
For a deeper clinical breakdown of causes, symptoms, and long-term outlook, see our Diastasis Recti Page.
Why Diastasis Recti Doesn’t Stay Local
A persistent abdominal split rarely exists in isolation.
In clients we work with, unaddressed diastasis recti is commonly associated with:
- Limited hip mobility, forcing the back extensors to overwork
- Upper crossed posture and shoulder rounding, feeding tension into the spiral line through the obliques
- Forward head posture, increasing pull through the superficial front line into the rectus abdominis
Over time, these compensations increase tension across the midline. The body relies more heavily on superficial muscles for stability, while deep core engagement becomes unreliable or inaccessible.
The result?
Pain shows up elsewhere—often far from the abdomen.
We’ve assessed diastasis recti in clients decades after childbirth, including one memorable case involving a nurse whose youngest child was 43 years old. She presented with plantar fasciitis and chronic back pain—and had a four‑finger separation she had never been told about.
Until that tension pattern is addressed, posture continues to degrade and symptoms persist.
Why “Just Strengthen Your Core” Often Backfires
Traditional ab exercises—sit‑ups, crunches, certain Pilates movements—tend to increase outward pressure on the linea alba when the deep support system isn’t firing correctly.
Instead of drawing the abdominal wall inward, these movements often pull the two sides of the rectus farther apart or prevent healing altogether.
Clinical evidence on isolated exercise programs for closing diastasis is currently limited and low quality. (PubMed Central 2021)
This isn’t a motivation issue or a discipline issue.
It’s a load‑management problem.
Until tension is reduced and the tissue is adequately supported, the body simply can’t organize strength effectively.
What Massage Therapy Can (and Can’t) Do
Massage therapy does not “close” diastasis recti.
What it can do—when applied intelligently—is reduce the forces that keep the split open.
In our work, that typically means:
- Myofascial release along the spiral and superficial front lines
- Working distal to proximal to create slack before addressing the abdominal wall
- Reducing excessive tone in tissues that are continually pulling on the midline
- Helping the nervous system downshift so deeper support patterns can emerge
Relief often shows up first as reduced back, neck, or shoulder pain—sometimes before clients are even aware of the abdominal component.
Some clinical studies have even shown improvements in separation and pain with myofascial approaches in postpartum populations. (Medicine 2023)
Massage creates the conditions for healing. It does not replace the need for protection or rehabilitation. (World J Psychiatry. 2024)
Why Bracing Is Non‑Negotiable (At Least at First)
If there’s one piece of guidance clients tend to resist, it’s bracing.
And yet, it’s often the most important part of recovery.
Because the linea alba behaves like connective tissue, it needs consistent support over time to adapt. For most people, that means:
- Wearing a supportive elastic brace (preferred)
- Or, at minimum, kinesiology tape
- For a period of six to twelve weeks
This isn’t a failure. It’s biomechanics.
I’ve worn a brace myself for twelve weeks—not because I had to, but to understand what I was asking clients to do. It’s inconvenient, yes. It’s also incredibly effective.
If a client could only choose one intervention, bracing would matter more than massage or exercise alone.
Where Physical Therapy Fits In
Massage therapy is an opening practice.
Physical therapy is a closing practice.
Once excessive tension is reduced and the tissue is protected, targeted exercises help retrain deep core engagement and restore functional strength.
We strongly recommend working with a physical therapist who specializes in diastasis recti and pelvic floor function. In many cases, we refer directly to trusted providers and coordinate care as needed.
The combination—manual therapy, bracing, and guided exercise—is far more effective than any single approach.
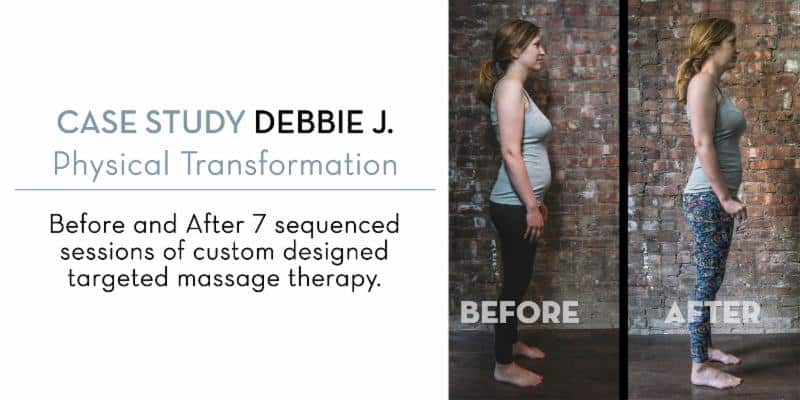
What Real Recovery Looks Like
Diastasis recti is not a one‑session fix.
Most successful recoveries involve:
- 4–7 sessions of targeted massage therapy
- 3–5 sessions with a specialized physical therapist
- Daily homework (often 10–15 minutes)
- Consistent bracing during the early phase
Knowledge and compliance account for most of the outcome. When clients understand what’s happening and why, results improve dramatically.
When to Look Deeper
If you’ve been dealing with persistent back pain, poor core engagement, or posture issues that never fully resolve—especially if you’ve ever been pregnant—it may be worth assessing whether an unrecognized diastasis recti is part of the picture.
We’ve seen these patterns linger for years. They don’t resolve on their own—but with the right approach, they can improve.
For a more clinical overview of diastasis recti and treatment considerations, you can also visit our full Diastasis Recti page.
If you’re unsure where to start, an in‑person assessment can help clarify whether massage therapy should be part of your care plan.
Last Modified: December 2025